
Academic Medical Institutions are challenged to advance discoveries that cure disease, educate and train the next generation of health leaders, and care for the most clinically complex patients. The academic bed tower of the future must create a strategic advantage in this mission by enabling the most efficient and effective care with flexibility and resiliency, and provide elevated experiences for patients, families, staff, and learners. As the largest, most expensive real estate on a quaternary health campus, the acute care tower must exemplify what is critical to an organization’s core purpose: patient satisfaction, staff efficiency and wellbeing, enhanced learning, and care outcomes.
For more than 30 years, HGA has been researching, prototyping, and advancing the ideal patient unit design. These designs have been implemented and tested, and what the post occupancy evaluations continue to show is the attributes of proximity, visibility, and divisibility are essential to the highest performing inpatient units for patients and staff.
Proximity
Proximity decisions have an impact on patient care time, effectiveness and efficiency of rounding, documentation time, safety, and overall effectiveness of the program. To understand current and optimize future operations, at the start of a project we ask questions about accommodating learners and rounding, deployed services such as imaging, use of robotics for materials management, medication distribution and storage, and patient transport. These highlight a key factor for optimal bed tower performance – proximity.

Case Study: Allina Health – Abbott Northwestern Hospital | New Teaching Hospital Patient Care Tower and Surgical Platform – Minneapolis, Minnesota
Abbott Northwestern Hospital is expanding their campus to meet the growing demand for high-acuity private beds and complex interventional procedures. HGA designed a highly integrative plan for a new Care Pavilion Tower addition along with phased removal and repurposing of aged facilities.
The project contains 192 new beds, 52 new interventional suites and 750,000 square feet of new construction on a tight, urban site in the center of an operating campus. The design combines three existing centers of excellence with the new interventional platform and bed tower, knitting them together into one cohesive new destination. The ideal outcome was to create a singular, seamless experience with services brought to the patient and centralized staff. Another HGA / Abbott collaboration, the Schulze Family Foundation Neurological Care ICU, demonstrated the significance of deploying imaging to the inpatient setting. This proximity improved outcomes through a 34% reduction in the time from imaging order to the start of the exam. With these proven outcomes, the client has now decided to deploy MRI, US, CT (another in ICU) and X-Ray to the floors for inpatient use in the new Patient Care Tower.
At the start of the project, the team tested scenarios of a single and a two-level interventional platform/PACU/Prep/Recovery to understand which one performed better against the project evaluation criteria. The new surgical platform is strategically co-located next to the existing Cardiovascular Center. The overall procedural center of the campus consists of 30 ORs in addition to CVOR, Hybrid, Cath, EP, Endo and IR. The entire procedural area shares Prep/Recovery and PACU, distributed over two floors. By co-locating these specialized groups, the Abbott team is better able to cross-cover and flex beds based on idealized staffing. The flexibility in the use of these spaces allows for a higher utilization of rooms, reducing the number of Prep/Recovery bays by 20%.
Steris Atlas WAV will be used on both the clean and soiled sides of the department. This system automates the transfer, wash and sanitization of surgical instruments. The robot will retrieve instrument racks from decontamination sinks and move and load them into washer/sanitizers without human interface. On the clean side, a robot will retrieve the now clean instrumentation and deliver it to prep/pack stations. Thus, several hot and heavy transfers are automated allowing staff to focus on quality control and throughput. This automation system will save staff 189 miles of travel per year, 79 hours of time, and 68,640,000 pounds of annual technical strain.
TUGs (Timed Up and Go) are planned to supplement team members in the materials management, dietary, linen and pharmacy departments. It is estimated that each TUG will alleviate the work of two staff members. This will allow current team members to move to roles where they can work to the top of their license.

Case Study: SSM Health – Saint Louis University Hospital | Master Plan, Replacement Hospital, and Ambulatory Care Clinic – St. Louis, Missouri
An urban infill project on Saint Louis University’s Medical School campus, the 825,000 square foot SSM Saint Louis University Hospital and 137,600 square foot ambulatory care center was designed as a destination for academic medicine, including retail amenities for patients and visitors, as well as medical students who populate the campus.
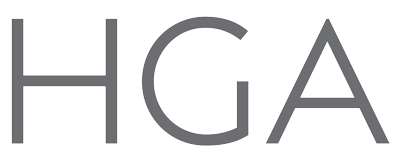
The facility houses 300 private, universal inpatient rooms to guarantee flexibility in room use and patient acuity. As the teaching hospital for Saint Louis University School of Medicine, the unique culture, rounding process, and academic requirements needed to be addressed in the planning.

Because attending physicians integrate patient care with learner education on every patient floor, the universal rooms are mirrored to create large collaboration alcoves outside each patient room, sized for teams of up to 20 people with direct line of sight to patients, equipped with charting and visualization technology to document and enhance learning, without disrupting normal patient care flow. Touch down areas for medical residents and faculty, and on-call spaces on every floor, also support the academic mission.
Visibility
Our evidence-based design research shows that improved site lines between caregiver and patient, combined with shortened travel distances through more efficient unit layouts and care protocols, led to increased patient satisfaction and enable value-added bedside and care activities, improved safety, and overall ROI. The next generation of HGA research will involve the integration of technology and its influence on caregiver bandwidth.

Case Study: Academic Medical Center | Confidential – Midwest
For this 36,000 square foot, 24-bed decentralized Medical Surgical Unit build-out, HGA used a series of Lean exercises and research tools to create an evidence-based unit design. User groups participated in activities that included peer-to-peer interviewing and space adjacency diagramming. At the same time, staff and patients on existing units were shadowed and interviewed. This baseline data created critical areas to measure (critical-to-quality metrics) such as patient satisfaction and staff efficiency that guided planning to, among other things, increase patient visibility and time providers spent at the bedside. The post occupancy evaluation demonstrated that the new unit design delivered the promised results and these results improved over time.
- Nurses spent roughly 45% of their time in patient rooms and at servers; a 6% increase per nurse
- 82% of time was spent on value-added activities such as providing direct care in patient rooms and coordination of care
- These are the highest performing units on the campus; estimated ROI from the new layout is projected to deliver a seven-year payback of the $6.25M renovation cost
Divisibility
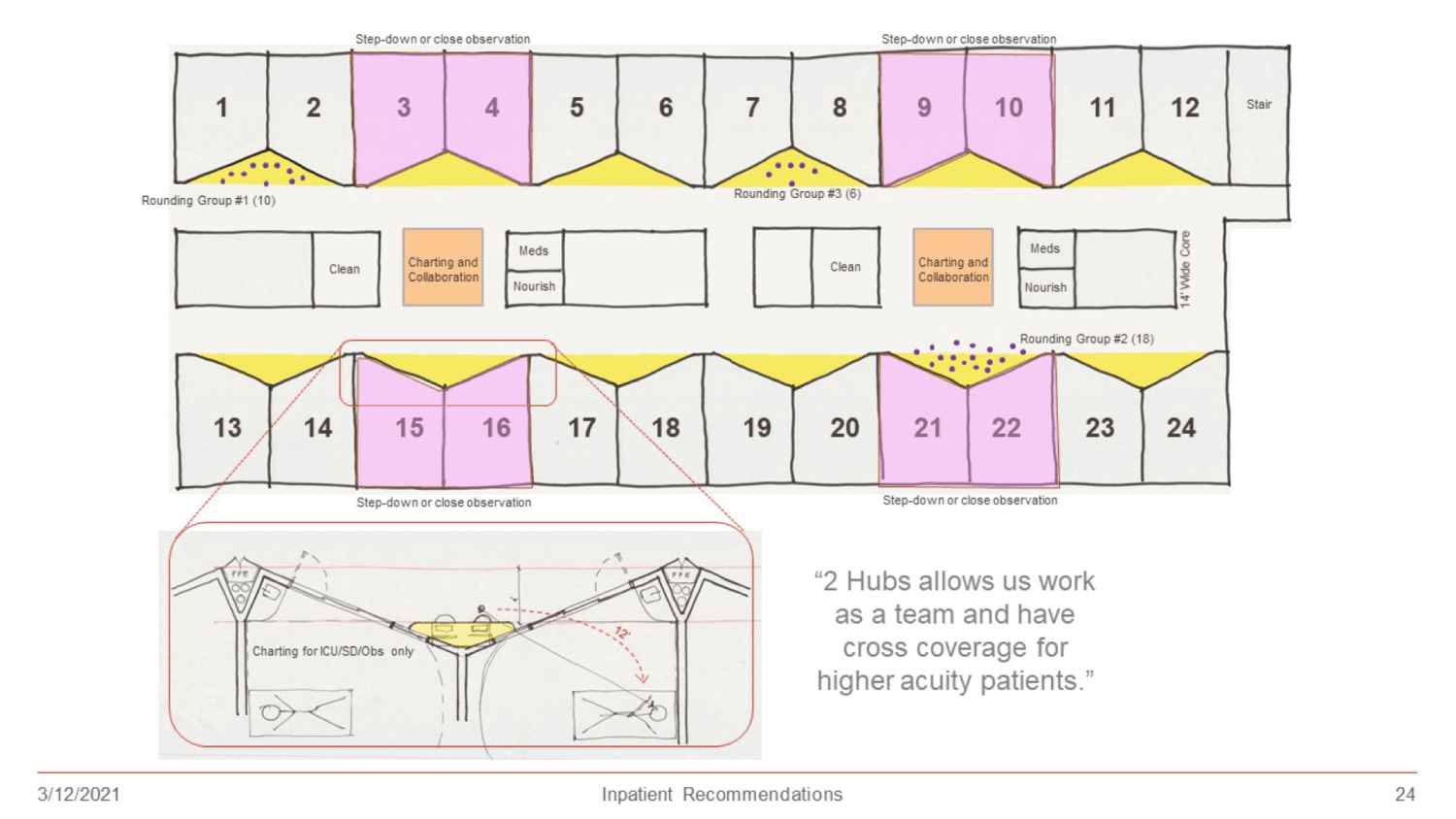
Flexibility in unit size is crucial to the academic bed tower of tomorrow. Strict classification of inpatient beds, whether by acuity or disease, results in small units that negatively impact the efficiency of services. So, to support flexibility, having units that are easily divisible makes a “more is more” solution for changing patient care demand. The key is to determine the right number of rooms, aligned to rounding and staffing ratios, and then create the most divisibility possible on the overall floor.
As shown above, acuity adaptable bed units require the right scale and combination of specialties to ensure a savings when co-locating. The data from an HGA bed tower project shows a 5% savings in square footage by co-locating Med/Surg and ICU on the same floor versus having separate units.

Case Study: MetroHealth | Campus Transformation and the Glick Center – Cleveland, Ohio
For MetroHealth’s new state-of-the-art teaching hospital, The Glick Center, HGA planners and Lean experts worked with hospital leadership to develop a program to replace aging facilities with new, more efficient ones. The resulting 800,000 square foot hospital is 110,000 square feet less than previously planned without sacrificing patient capacity or future growth projections.
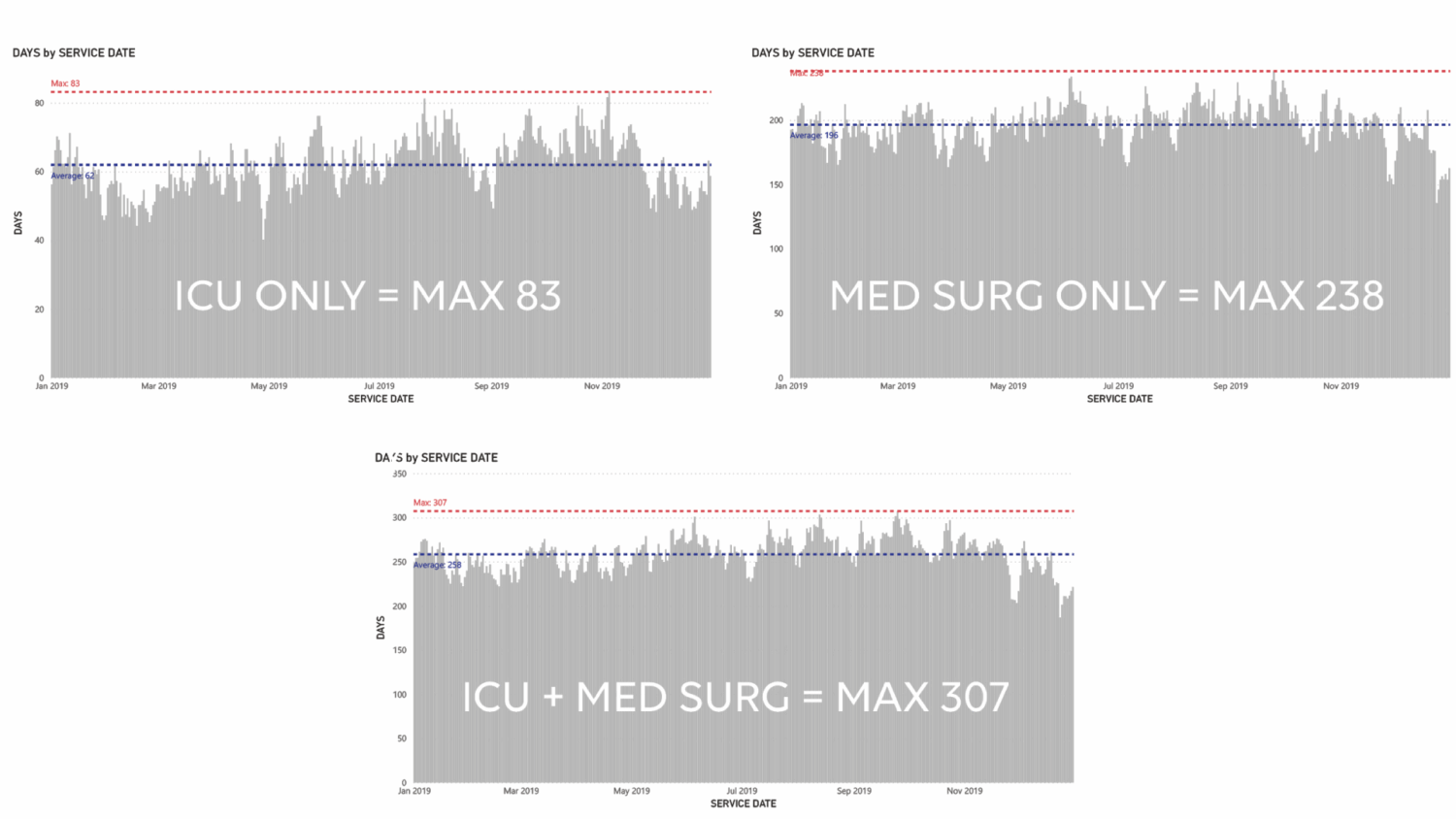
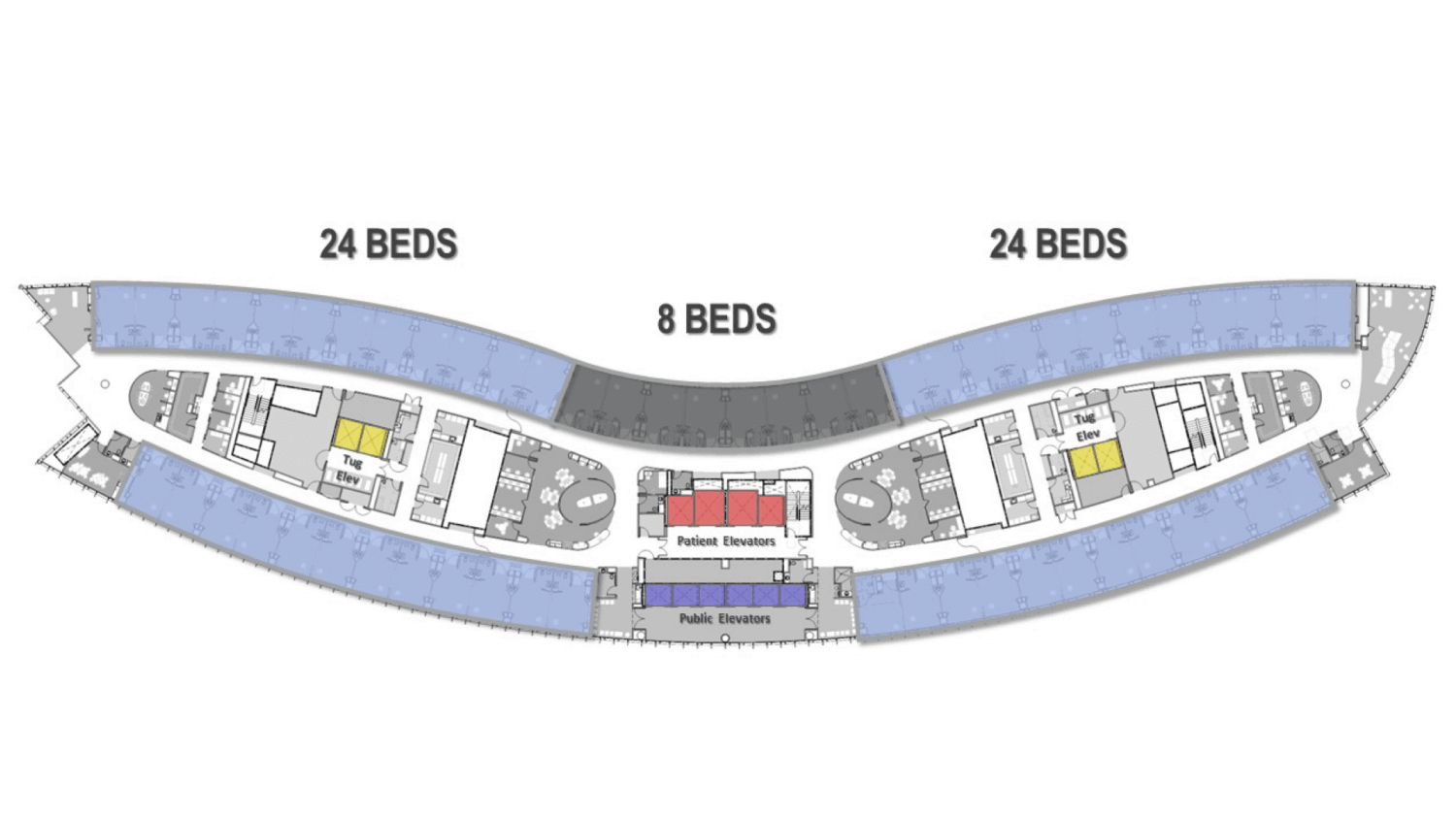
HGA updated the shape of the building to enable a thinner core that increases visibility across the core and the continuous rail of rooms on one side. The inpatient unit is divisible in multiple ways to set up 8-bed units to align with care needs.
- The thinner core increases visibility across the core.
- The inpatient unit is divisible in multiple ways to set up multiple units of 8-beds which configure as:
Two 24-bed units | Four 12-bed units | Three 16-bed units | Three 8 + 8-bed units - The tapered floor plate provides larger staff support towards the center supporting additional functions, with smaller staff support areas towards the edges to increase proximity to patients. The central supply core is flexible to accept robotic medication and supply delivery in the future. A central elevator core separates different flows, public to the front and staff and service to the back.
The inpatient platform design addressed the core requirements of Visibility, Divisibility and Proximity – and the additional need for ultimate flexibility. The resulting “Process Neutral” Design approach created a neutral care platform that can easily change to support current and unforeseen processes 50 years into the future. Bringing intensive care units into the new tower and repurposing their location in the existing Critical Care pavilion to establish a new Women’s and Children’s Pavilion, allowed for the development of 288 universal, variable acuity Medical/Surgical/Intensive Care rooms – assuring maximum flexibility for patient aggregation in the future. The approach equated to a savings of over $75M from the previous master plan estimates, improving MetroHealth’s ability to deliver on four core values—Human Experience, Clinical Outcomes, Energy & Environment, and Space Optimization.

Case Study: UPMC Presbyterian Hospital | Comprehensive Plan – Pittsburg, PA
Having completed the UPMC system master plan, HGA is now in the final stages of design for the new 853,000 square foot Presbyterian tower that supports Centers of Excellence. The tower will be the new front door of the hospital and includes a 644 beds and 40-room surgery addition/renovation incorporating the latest in innovative surgical technology. The state-of-the-art tower is based on the evidence-based design features of the HGA-designed inpatient prototype and advances them into the future of medicine.
In the new hospital, inpatient floors are organized around disease management rather than by acuity. Adjacent units on the same floor mix acuity, co-locating complementary service lines by disease type and nursing competencies. Disease management aggregation enhances nursing care around the highest clinical outcomes, as well as co-locating all patients in the service line together, at least 85% of the time. This is projected to reduce bed demand by 40 beds compared to a model that co-locates by acuity level.
ADDITIONAL CONSIDERATIONS
Flexibility Through Prefabrication
The emerging trend in the design and construction industry is the push toward more modular and prefabricated construction that improves quality while reducing cost. Prefabrication reduces infrastructure constraints and makes it easier to evolve, redesign, or repurpose spaces for different use or more efficient operational models over time. Renovations can be done more quickly and for less cost than traditional designs. Scalability is improved, so clinical areas are more efficiently subdivided by need without artificial barriers and staff areas can be worked on without disruption to clinical areas.
Prefabricated elements (whether panels, components, pods or modules) are often of higher and more consistent quality than ones constructed in the field because they are built in controlled conditions and inspected for quality during manufacturing and at installation.
To best support efficient and effective care while enhancing patient, staff, and learner experiences, the future academic bed tower will feature the right combination of proximity, visibility, and divisibility in planning. Our research and proven results show that this method can result in increased performance and ROI for any bed tower, no matter the location, patient population, or mix of services.